(USMLE topics) Alcoholic fatty liver, alcoholic hepatitis, and cirrhosis: Signs and symptoms, risk factors, pathophysiology, complications, diagnosis and treatment. This video is available for instant download licensing here: https://www.alilamedicalmedia.com/-/galleries/all-animations/digestive-system-videos/-/medias/012159d6-87f0-425d-bd0d-37b284ff287a-alcoholic-liver-disease-narrated-animation ©Alila Medical Media. All rights reserved. Voice by : Marty Henne Support us on Patreon and get early access to videos and free image downloads: patreon.com/AlilaMedicalMedia All images/videos by Alila Medical Media are for information purposes ONLY and are NOT intended to replace professional medical advice, diagnosis or treatment. Always seek the advice of a qualified healthcare provider with any questions you may have regarding a medical condition. Alcoholic liver disease is liver damage caused by alcohol abuse. The risk of developing liver disease correlates with the amount and duration of alcohol use. Daily drinking poses a higher risk than binge drinking. Other risk factors include gender, genetics, and obesity. Alcoholic liver disease includes 3 disorders that develop in sequence: alcoholic fatty liver, alcoholic hepatitis, and cirrhosis. Alcoholic fatty liver is accumulation of liver fat as a result of alcohol use. The liver is usually enlarged but not tender. There are often no symptoms and the condition can be reversed if the patient stops drinking. Alcoholic hepatitis is liver inflammation. Symptoms can range from mild to severe and may include fever, jaundice, fatigue, and a tender, painful and enlarged liver. Cirrhosis is when a large amount of hepatic tissue is permanently replaced with non-functional scar tissue, known as fibrosis. Symptoms range from those of alcoholic hepatitis to those of end-stage liver disease. The liver eventually shrinks. Cirrhosis cannot be reversed. The liver is the major site of alcohol metabolism. Two main pathways are involved: alcohol dehydrogenase, ADH; and cytochrome P-450 2E1, or CYP-2E1. ADH converts alcohol to acetaldehyde. A second enzyme, acetaldehyde dehydrogenase, ALDH, then metabolizes acetaldehyde to acetate. People who have low levels of ALDH are more susceptible to toxic effects of acetaldehyde. Both of these reactions convert NAD+ to NADH. An increased NADH/NAD+ ratio promotes fatty liver by inhibiting fatty acid oxidation and stimulating fatty acid synthesis. In addition, acetaldehyde also promotes production of enzymes involved in fatty acid synthesis, and inhibits expression of enzymes implicated in fat oxidation. Alcohol use has also been shown to reduce export of fat from the liver. All these events lead to fat accumulation in hepatic cells. Chronic alcohol use upregulates the CYP-2E1 pathway. This pathway generates harmful reactive oxygen species, which can damage proteins and DNA. The effect is exaggerated in patients who are deficient in antioxidants due to malnutrition. Chronic alcohol exposure also activates hepatic macrophages, triggering inflammation. In addition, acetaldehyde can bind to cellular proteins, forming so-called adducts that are seen as foreign antigens by the immune system, provoking the body’s inflammatory attacks. Chronic inflammation and subsequent attempts at tissue repair lead to formation of scar tissue. As a result, the liver internal structure is disrupted, impairing its functions. Scarring of liver tissue also obstructs blood flow, causing high blood pressure in the portal vein that brings blood from the intestine to the liver. As liver functions decline, toxins that are normally removed by the liver can now reach the general circulation and pass into the brain, producing symptoms such as confusion, drowsiness, tremor, or even coma, in a condition known as hepatic encephalopathy. Portal hypertension may cause variceal bleeding, enlarged spleen, and abdominal distension. Diagnosis is usually based on signs of liver dysfunction, other symptoms related to alcohol use, history of heavy drinking, liver function tests and complete blood count. Abstinence is the best treatment. Supportive care includes good nutrition and vitamin supplements. Corticosteroids may be used to reduce inflammation but their effectiveness is till debatable. Liver transplantation may be considered for abstinent patients with severe liver damage.
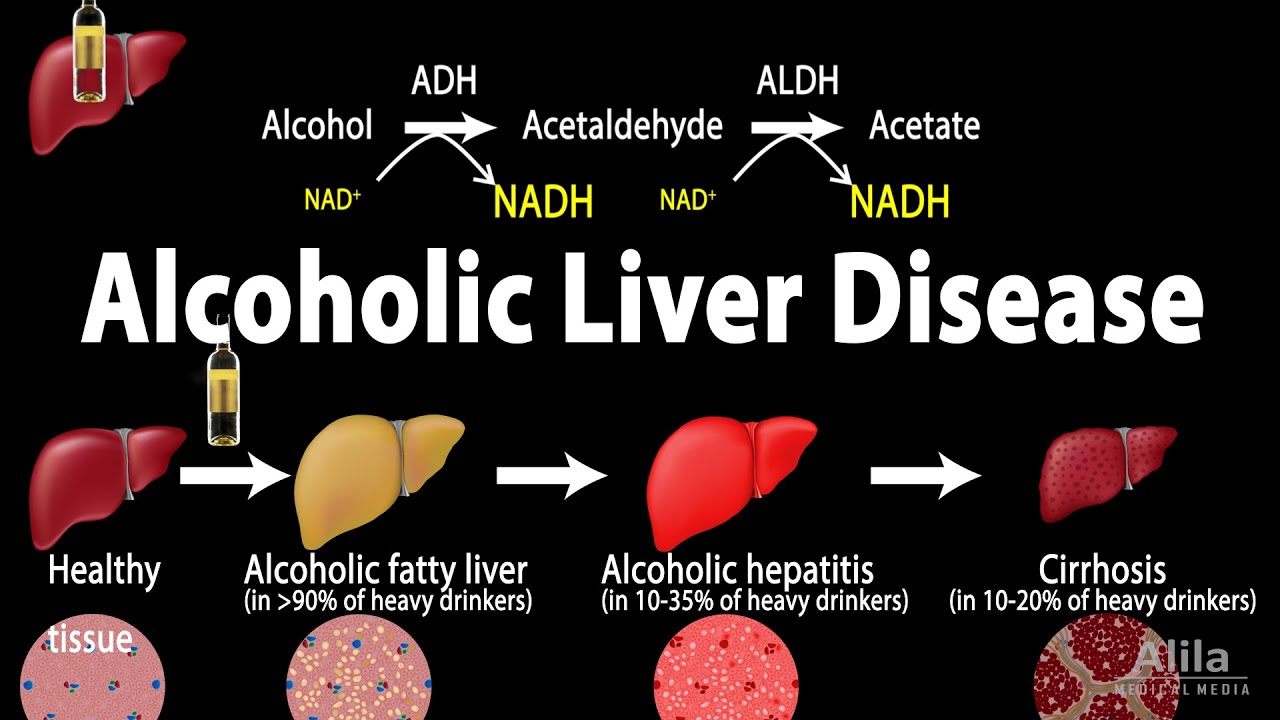
Alcoholic Liver Disease, Animation
You Might Also Like

Dermatology Video – 1

Preventive Medicine Video – 3

Dumbbell Chest Workout (INCOMPLETE WITHOUT THIS!)

5 tips for gaining muscle – Fitness, Bodybuilding & Nutrition

5 Reasons You NEED to LIFT LIGHT Weights!! (Important)

URINE ANALYSIS: Presence of PROTEIN in urine

How to check man sperm count for fertility at home
Menopause and Weight Gain Simplified | Women’s Health

Arm Workout Tips | Hammer Curls | Biceps Workout

Total Body Strength Training Workout | Weight Training Routine for Men and Women | HASfit

How To: Standing Lat Pushdown (Cable Machine)
10 Mind Blowing Creatine Benefits

Define Me Sport
Low Sperm Count Cure | 3 magical points
Parts of the Brain-Human Brain Structure and Function

Intro Anatomy 3 Abdominal Cavity 1

Definition Fitness – Building Dolph

Cycling Video – 4

Tuberculosis (TB) symptoms animation

What Causes Hair Loss | What Causes Alopecia Areata | Cure To Baldness

What is Fish Oil? Omega-3 Benefits & Side Effects Review by Guru Mann

These Are The Symptoms and Signs You May Have a Blood Clot in Your Leg

What Is Happening When Acne Forms? Does This Knowledge Help Prevent Acne?

Isotretinoin-exposed pregnancies still occur

CONCENTRATION CURLS for PEAK on BICEPS! (Hindi / Punjabi)

How to Council Your Acne Patients on Isotretinoin – Julie Harper DERM2017

Medicine Ball Back Extension
Post Workout Nutrition

What to EAT AFTER EXERCISE (Post Workout)! (Hindi / Punjabi)

Cardio-Thoracic Physiotherapy Video – 1
Human anatomy 3d animation

Intermittent Fasting & Fasting Video – 16

WHAT I EAT IN A DAY | WEIGHT LOSS MEAL PLAN FOR WOMEN

How to improve endurance and core strength | Soccer training drill | Nike Academy

What is BMR and how does it effect my HCG diet?
Complete 20 Min ABS Workout – Gym Body Motivation

Geriatric Physiotherapy Video – 14

Breads For Your Weight Loss Diets

Side Effects of Omega 3 Supplements | BestFishOill.com

HGH, Growth Hormones & Plant Hormones Video – 41

Physiology Of Sports & Sports Medicine Video – 3
