How serum potassium levels affect resting membrane potential and cardiac action potential; ECG (EKG) changes in hyperkalemia. How hyperkalemia causes bradycardia. Electrolytes disorders This video is available for instant download licensing here: https://www.alilamedicalmedia.com/-/galleries/narrated-videos-by-topics/ekgecg/-/medias/0e40597c-5219-4950-abbe-aa1583b53ed9-hyperkalemia-narrated-animation ©Alila Medical Media. All rights reserved. Voice by: Sue Stern. Support us on Patreon and get FREE downloads and other great rewards: patreon.com/AlilaMedicalMedia All images/videos by Alila Medical Media are for information purposes ONLY and are NOT intended to replace professional medical advice, diagnosis or treatment. Always seek the advice of a qualified healthcare provider with any questions you may have regarding a medical condition. Hyperkalemia refers to abnormally high levels of potassium in the blood. The ratio of INTRAcellular to EXTRAcellular potassium is important for generation of action potentials and is essential for normal functions of neurons, skeletal muscles and cardiac muscles. This is why potassium levels in the blood are strictly regulated within a narrow range between 3.5 and 5mmol/L. As the normal daily dietary intake of potassium varies widely and can be as much as 100mmol a day, the body must keep blood potassium levels within the normal limits. This is achieved by 2 mechanisms: – Excretion of potassium through the kidneys and intestines – Shifting of potassium from the extracellular fluid into the cells by the sodium/potassium pump. The pump is mainly regulated by hormones such as insulin and catecholamines. Hyperkalemia is defined as a serum potassium concentration HIGHER than 5mmol/L. Hyperkalemia may result from decreased excretion, excessive intake, or shift of potassium from INSIDE the cells to EXTRA-cellular space. The most common scenario is a RENAL INsufficiency combined with excessive potassium supplements OR administration of certain drugs. Impaired kidney function is most prominent Mild hyperkalemia is often without symptoms, some patients may develop muscle weakness. Slow or chronic increase in potassium levels is less dangerous, as the kidneys eventually adapt by excreting more potassium. Sudden onset and rapid progression of hyperkalemia can be fatal. Primary cause of mortality is the effect of potassium on cardiac functions. As potassium levels INcrease in the EXTRAcellular space, the MAGNITUDE of potassium gradient across the cell membrane is REDUCED, and so is the ABSOLUTE value of the resting membrane potential. Membrane voltage becomes less negative, moving closer to the threshold potential, making it EASIER to initiate an action potential. The effect this has on excitability of myocytes, however, is complex. While initial changes seem to increase myocyte excitability; further rise of potassium has the OPPOSITE effect. This is because the value of membrane potential at the onset of an action potential DETERMINES the number of voltage-gated sodium channels activated during depolarization. As this value becomes less negative in hyperkalemia, the number of available sodium channels DEcreases, resulting in a SLOWER influx of sodium and subsequently SLOWER impulse conduction. ECG changes produced by hyperkalemia follow a typical pattern that correlates with serum potassium levels: peaked T-wave, P wave widens and flattens, PR interval lengthens, QRS complex widens and eventually blends with T-wave. Diagnosis on the basis of ECG alone very difficult. Acute hyperkalemia must be suspected in any patient having new bradycardia or conduction block, especially in those with renal problems. Severe hyperkalemia is treated in 3 steps: – Calcium infusion is given to rapidly REVERSE conduction abnormalities. – Insulin to stimulate the sodium/potassium pump, promoting INTRA-cellular shift – Hemodialysis to remove potassium
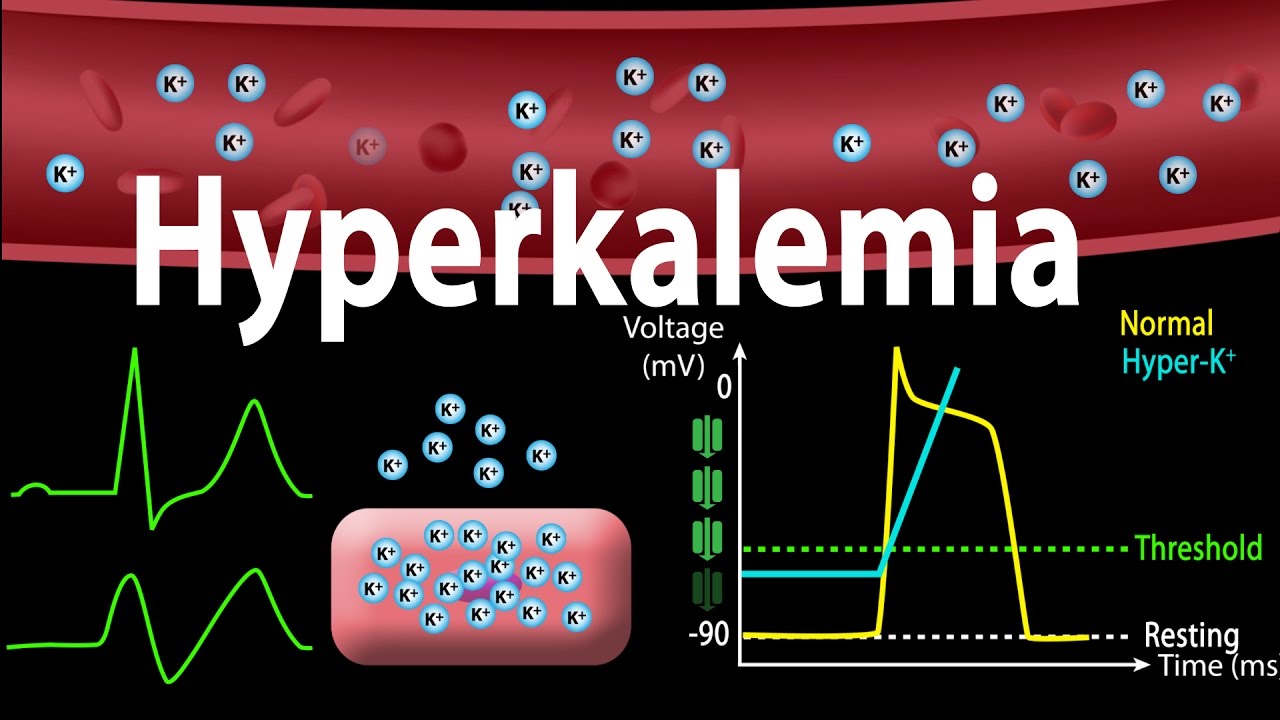
Hyperkalemia: Causes, Effects on the Heart, Pathophysiology, Treatment, Animation.
You Might Also Like
The Suprising Facts on How and Where Exactly Thyroid Hormones Are Made

Breathing Exercise For Strong Lungs
Amino Acids: What are they? What do they do?

Preacher Curl Machine or Biceps Curl Machine – HASfit Machine Exercises – Machine Exercise

Menopause Nutrition Video 1
Structure of Bone|Anatomy of Bone|3D Animation|Biology

This Surprising Test Reveals Your True Body Type | Know your body for better result – in hindi
Signs You Have An Enlarged Liver
What is SEMEN? What does SEMEN mean? SEMEN meaning, definition, explanation & pronunciation

Hormones and Men’s Health

What Is Arthritis Types Of Arthritis – Top Home Health Tips For Arthritis Treatment

Hyperextension on Swiss Ball

Hologic Sahara Bone Densitometer
Human Body Video – 2

Seated & Standing Calf Presses

Will Rice And Potato Make You Gain Weight

KOREAN BODYBUILDERS : The best Genetics in the WORLD?

How to Pistol Squat – 4 Beginner Progression Steps – Tapp Brothers

Cardio-Thoracic Physiotherapy Video – 4

Heart Disease | Health | Biology | FuseSchool

Can you get pregnant after an ectopic pregnancy | Quick Question

How To: Standing Barbell Calf Raise

Aroma Oils Video – 1

Intec Pharma – Drug Delivery system, produced by Virtual Point

How to make delicious lactation cookies (to help boost your milk supply)

CONCENTRATION CURLS for PEAK on BICEPS! (Hindi / Punjabi)
Dumbel 1 arm lying triceps extension
5 KILLER Chest Exercises With NO BENCH (GRUUUUESOME!!)

Fat Loss, Weight Loss Video – 30

Arm Workout Tips | Hammer Curls | Biceps Workout

Spa Types Video – 2

Human Physiology – Hormonal Regulation of Male Reproduction

5. Program Exercise - Program Exercise〈Your First PLC (17/19)〉
Endocrine System Diabetes And Asanas Video – 5

deamination and the liver.
Can vitamin supplements cause liver damage ?

Thyroid Animation

Physical Fitness Defined | The Definition of Physical Fitness

Radiology Video – 4
Pre Workout Nutrition Video – 2

Pectoralis Pushups-4
