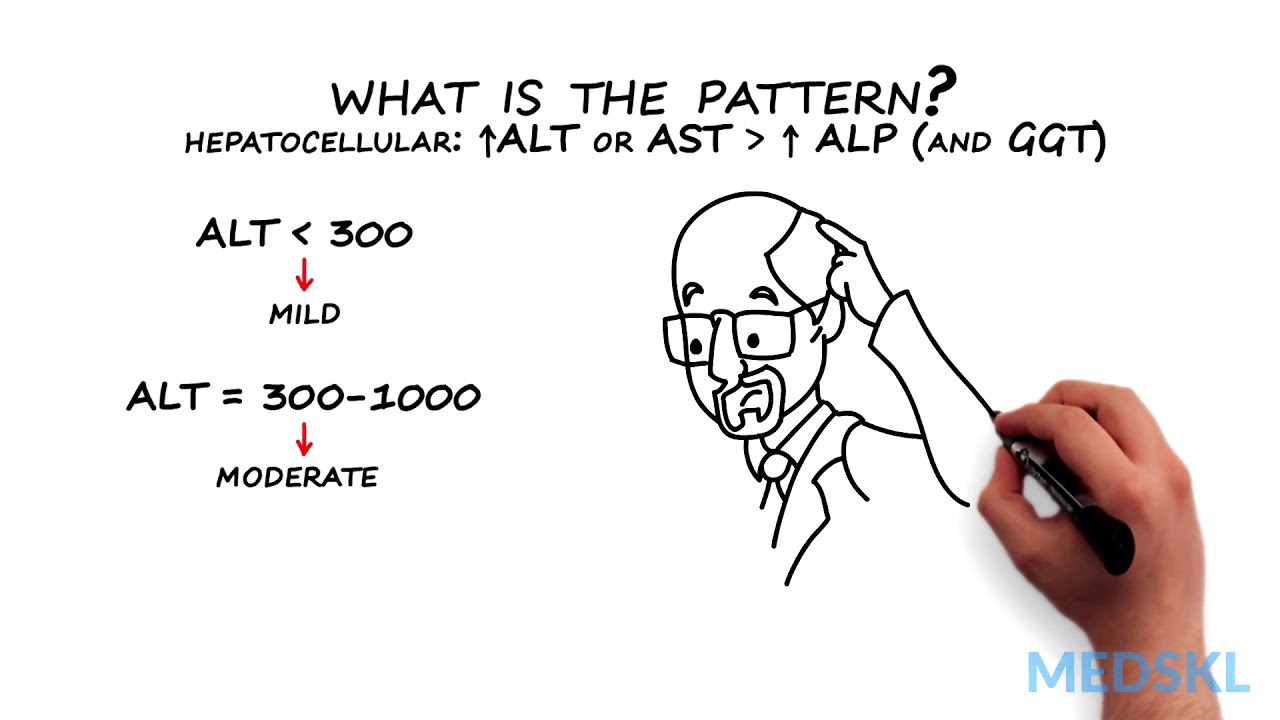
Abnormal liver tests occur frequently. Liver enzymes are frequently confused with liver function tests. This module will help distinguish the two. It is important to be able to assess the test results in light of the patient’s presenting complaint, risk factors and condition. This module will also cover an approach to patients with abnormal liver test results. medskl.com is a global, free open access medical education (FOAMEd) project covering the fundamentals of clinical medicine with animations, lectures and concise summaries. medskl.com is working with over 170 award-winning medical school professors to provide content in 200+ clinical presentations for use in the classroom and for physician CME. Gastroenterology – Abnormal Liver Tests Whiteboard Animation Transcript with Kelly Burak, MD https://medskl.com/module/index/abnormal-liver-tests INTRODUCTION Liver tests or liver enzymes, sometimes incorrectly call liver “function” tests, refer to AST, ALT, ALP, and may include GGT. Abnormal values are often found on routine blood tests and indicate liver injury. Bilirubin, albumin and prothrombin time (or INR) are better tests of the function of the liver and are the LFTs. How to Interpret Abnormal Liver Tests A patient with abnormal liver tests can present in a number of different ways or can be completely asymptomatic.1,2,3 While a clinical assessment focused on risk factors and stigmata of liver disease remains key, the pattern of liver enzyme elevation will guide the differential and workup. 1. Take a look at which enzymes are elevated. A rise in ALT and/or AST that is proportionally higher than ALP indicates a hepatocellular pattern of injury,1 while A rise in ALP, confirmed to be from liver by an abnormal GGT, indicates a cholestatic pattern.1 2. What is the pattern? If the pattern of injury is cholestatic – that is the ALP (and GGT) rise > ALT or AST – you will need to obtain a dedicated ultrasound of the liver and biliary tree to look at the bile ducts Dilated bile duct indicate extrahepatic cholestasis and an ERCP may be needed for diagnosis and therapy Normal bile ducts indicate intrahepatic cholestasis, and a liver biopsy may be required if the cause is not identified by history or other investigations, such as an anti-mitochondrial antibody or MRCP If the pattern of injury is hepatocellular – that is the ALT or AST rise is greater than ALP (and GGT) – determine severity using the ALT level An ALT of <300 is mild and 300-1000 correspond to moderate liver disease.1 These can be acute or chronic and unfortunately the differential diagnosis is broad Non Alcoholic Fatty Liver Disease (NAFLD) is the most common cause of mild elevation4,5 Alcoholic liver disease is associated with an AST that is often 2-3 times higher than the ALT, but alcohol or NAFLD rarely cause the ALT to be <3001,4,5 Further evaluation and testing will be guided by your history and clinical suspicion If ALT >1000 there is SEVERE liver injury which is always acute and symptomatic. These patients are at high risk of acute liver failure.1,3 If you see these values, think and test for the following: Drugs – especially acetaminophen overdose; Viruses – Hepatitis A through E, HSV, CMV, VZV; Ischemia from Budd-Chiari Syndrome or shock; Autoimmune Hepatitis; Wilson’s Disease; and if the patient is pregnant or recently postpartum, HELLP syndrome or acute fatty liver of pregnancy (AFLP)1,3 Quick recognition and diagnosis can guide appropriate management in these patients
Gastroenterology – Abnormal Liver Tests: By Kelly Burak M.D.
You Might Also Like
Kidney disease – Causes and treatment of kidney failure

Atenolol or Tenormin Medication Information (dosing, side effects, patient counseling)

Quality of Supplements – Dr. Mark Menolascino MD (307)732-1039

7 Powerful Fruits To Lose Weight And Burn Belly Fat Instantly
Best Diet Plan To Lose Belly Fat in 4 Weeks (Top 9 Fat Loss Foods)
Andropause: Treating Male Hormone Imbalance Naturally (Male Menopause)
How to do Cable Bent Over Triceps Extensions? #91

Diseases Caused by Malnutrition – SCURVY, RICKETS, BERIBERI, PELLAGRA

Pregnant? Help Protect Your Baby from Whooping Cough

What’s happening in my uterus?!

♥ 3 Best Exercises For Increasing Blood Flow & Circulation To Your Legs – by Dr Sam Robbins

What’s the Best Cardio for Thin Thighs? | Thighs Workout
What is a renal function test ?

Foods For Gut Health & Digestion | Nutrition & Wellness | Healthy Grocery Girl

Arthritis Nutritional Tips

Top Four Bodybuilding Supplements Worth Your Money @hodgetwins

Hypotension Meaning
The Ayurvedic Body Types and Their Characteristics (Vata, Pitta, Kapha)

Sleep Medicine Video – 3
Thyroid Blood Tests

How To Sprint – Pt. I

Sex Psychiatry Video – 3

Overweight & Obesity Video – 3

Pre & Post Workout Nutrition Guide – How To DIY TV
Muscle Definition – Does Your Training Matter? 8 minute explanation

Should I use Minoxidil / Rogaine for my hair loss? | #AskNatureCrazyShow – Episode 4
How The Body Uses Food – You Are What You Eat
Diarrhea, Definition, Symptoms, Causes, Natural Remedies

Anesthesiology Video – 3

Intermittent Fasting & Fasting Video – 16

Exercise Anatomy Video – 3

Stability Ball Hyper Extension Training Exercises

Forearm Training Tips
Testosterone & Androgenic Effects Video – 11
Legal Psychology Video – 1

Dead Lift-2
Human Body Systems Video – 2
Lunge dumbbell row: upper back, triceps, lats & hamstrings workout with weights

Weight Training Video – 4

Pilates Video – 5

Reverse back extension
